Adenomatoid odontogenic tumor associated with maxillary premolars
 The following is a synopsis of the article, “Adenomatoid odontogenic tumor associated with impacted maxillary premolars: report of 2 cases,” which appears in the May/June 2026 issue of General Dentistry. Read the full article here.
The following is a synopsis of the article, “Adenomatoid odontogenic tumor associated with impacted maxillary premolars: report of 2 cases,” which appears in the May/June 2026 issue of General Dentistry. Read the full article here.Adenomatoid odontogenic tumor (AOT) is a benign, slow-growing, painless lesion found in tooth-bearing sites of the jaws.1 Because approximately two-thirds of confirmed cases have arisen in the maxilla, involved younger females, and exhibited focal radiographic calcifications, AOT is sometimes characterized as the “two-thirds tumor.”1,2 The lesion most commonly affects maxillary canines and is typically observed on radiographs as a well-circumscribed, teardrop-shaped radiolucency containing an embedded tooth.3 In the May/June issue of General Dentistry, Abdul-Wasay et al report two atypical cases associated with impacted maxillary premolars, including an AOT in a young man and a lesion affecting two teeth.
Case 1
A 19-year-old man who sought routine dental evaluation was unaware of a firm, nontender swelling in the maxillary right buccal vestibule that extended from the canine to the second premolar. There was no palatal expansion. A panoramic radiograph showed a 38 × 24-mm corticated, unilocular, teardrop-shaped radiolucency containing an impacted and apically positioned maxillary right first premolar adjacent to small calcified structures. Cone beam computed tomographic images showed multiple snowflake-like calcifications (Fig 1). The radiographic differential diagnosis included AOT, dentigerous cyst, odontogenic keratocyst, calcifying odontogenic cyst, ameloblastoma, and calcifying epithelial odontogenic tumor.

Fig 1. Case 1. CBCT images of the cystic lesion showing multiple snowflake-like calcifications. A. Sagittal view. B. Axial view. C. Coronal view.
The patient was referred for excisional biopsy, during which the lesion and the tooth were separated from the surrounding bone and easily removed en masse with a curette, leaving a bony defect that was irrigated and closed with absorbable sutures (Fig 2). Histopathologically, the lesion displayed abundant spindle cells with minimal fibrous stroma and scant areas of eosinophilic material; well-circumscribed islands of epithelium arranged in whirling nests and rosettes; small duct-like structures lined by cuboidal and columnar cells; and variable focal aggregates of basophilic calcifications. The diagnosis was follicular AOT.
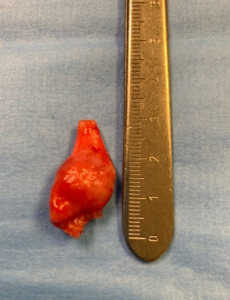
Fig 2. Case 1. En masse removal of the lesion.
Case 2
An 8-year-old girl presented for evaluation of buccal expansion in the maxillary left posterior area as well as mobility of the primary canine, first molar, and second molar. A panoramic radiograph revealed a 38 × 38-mm corticated, slightly teardrop-shaped radiolucent lesion containing 2 unerupted maxillary left premolars (Fig 3). Root resorption of adjacent teeth was observed. The patient was referred for biopsy. During the procedure, a scant amount of serous-like fluid was aspirated from the lesion. A full-thickness flap revealed cortical thinning that facilitated buccal alveolar entry. Soft tissue aggregates were curetted, and histopathologic findings, similar to those described in case 1, established a diagnosis of follicular AOT.
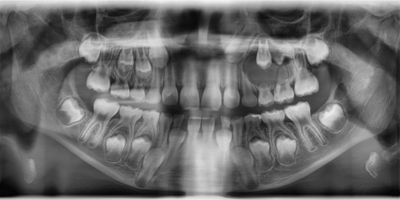
Fig 3. Case 2. Panoramic radiograph showing a cystic lesion enveloping 2 maxillary premolars.
Discussion
AOT is an asymptomatic, benign, indolent odontogenic lesion predominantly affecting younger females and associated with a single impacted permanent tooth, usually the maxillary canine.2 Involvement of primary teeth is unusual, and premolar involvement has been recorded only occasionally.4 In both presented cases, the radiologic and histopathologic findings of the expansile lesions, which affected maxillary premolars, were consistent with follicular AOT. The inclusion of 2 or more teeth within an AOT, as seen in case 2, is extremely rare.5
In most cases, an AOT manifests clinically as a painless buccal or labial alveolar expansion with normal mucosal color.3 Radiographically, AOT usually appears as a well-circumscribed, somewhat teardrop-shaped unilocular radiolucency with corticated borders. It may contain multiple snowflake-like inclusions, and root resorption has been reported in 17% of cases.3 Displacement of contiguous teeth is common. Microscopically, AOT is composed of spindle cells admixed with duct-like structures, anastomosed strands of epithelial cells arranged in whirling nests and rosettes, amorphic eosinophilic material, and a thick fibrous capsule encircling the crown of a tooth.2 Differing numbers of irregular-shaped calcific structures may be seen, including a variant with concentric layering, referred to as a Liesegang pattern.6
Management of AOTs consists of conservative surgical enucleation and curettage, as the tumor’s fibrous encapsulation and minimal propensity for invasion ensure an excellent long-term prognosis.3 At the 2-week follow-up examination, the patient in case 1 presented with a 2 × 2-mm dehiscence, occasionally observed as a self-resolving sequela.7 The 6-month postoperative radiograph revealed osseous healing without evidence of disease recurrence, in agreement with expert consensus that appropriate surgical management in most cases of AOT consists of enucleation and curettage.8 Despite several attempts at contact, the patient in case 2 was lost to follow-up.
Conclusion
This report documents 2 less common presentations of AOT, which is usually associated with a single impacted maxillary canine in younger females. The tumor has an excellent prognosis when treated with enucleation and curettage, and lesional recurrence is uncommon. Malignant transformation of AOT has not been reported in the literature to date.
References
1. Sam SS, Fitzpatrick SG, Bhattacharyya I, Cohen DM, Islam MN. Adenomatoid odontogenic tumor: a series of 28 cases from a biopsy service. Quintessence Int. 2022;53(3):260-269. doi:10.3290/j.qi.b2218723
2. Vargas PA, Gomes CC, Upadhyaya J, van Heerden WFP. Adenomatoid odontogenic tumour. In: WHO Classification of Tumours Editorial Board, ed. Head and Neck Tumours. Part A. WHO Classification of Tumours. 5th ed. Vol 9. International Agency for Research on Cancer; 2024:331-332.
3. Chrcanovic BR, Gomez RS. Adenomatoid odontogenic tumor: an updated analysis of the cases reported in the literature. J Oral Pathol Med. 2019;48(1):10-16. doi:10.1111/jop.12783
4. Kalia V, Kalra G, Kaushal N, Sharma V, Vermani M. Maxillary adenomatoid odontogenic tumor associated with a premolar. Ann Maxillofac Surg. 2015;5(1):119-122. doi:10.4103/2231-0746.161118
5. Tsaknis PJ, Carpenter WM, Shade NL. Odontogenic adenomatoid tumor: report of case and review of the literature. J Oral Surg. 1977;35(2):146-149.
6. Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu QX. Adenomatoid odontogenic tumor: biologic profile based on 499 cases. J Oral Pathol Med. 1991;20(4):149-158. doi:10.1111/j.1600-0714.1991.tb00912.x
7. Ferreira KRH, Meira CLS, de Castro Moraes J, Daroz BG, de Souza LL, Xavier TB. Adenomatoid odontogenic tumor in the anterior mandible: a case report. J Oral Diagn. 2022;7:e20220203. doi:10.5935/2525-5711.20220203
8. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Elsevier; 2023:718-720.